
Christ Trumps Psychology & Psychiatry
My Decision to Pursue Psychology
As a teenager, I decided to pursue a career in psychology. If I could do things over, I would turn to Christ over psychology.
When I was a kid, I had come down with a bad case of obsessive-compulsive disorder, and it was around that time that my interest in psychology was triggered. So, in pursuing psychology, I fulfilled the cliché of a person who enters the field because of personal unresolved psychological issues, hoping to find a solution and then share it with others. I remember when I was getting into psychology, associating it in my mind with a certain “darkness.” My mother wanted me to go into nursing instead. But I persisted at studying psychology in college.
Initially, I had aspirations of becoming a professor or a researcher. Therapy didn’t have much appeal for me, either for the giving end or receiving end. I didn’t see talk therapy as particularly effective, and from a personal standpoint, I didn’t like the idea of spilling personal matters to a stranger. I figured all one needs is to obtain knowledge of the human psyche and to discover practical solutions for one’s problems and then to apply these and move on. Over the years I became increasingly on the lookout for knowledge.
How I Overcame OCD (Initially), Anxiety, and Asocial Tendencies
As it turned out, I cannot credit the mental health field with having helped me overcome three of my major issues at the time. It’s not to say that they never offer good advice, because you can find good advice. Case in point, in regards to dealing with OCD, the book Brain Lock has some good advice to offer – not identifying with the intrusive thoughts and viewing them from the viewpoint of an independent spectator. However, I didn’t draw on anything I learned from psychology to achieve victory in three problem areas.
The anxiety issue I had was resolved by me basically applying logic, having a change of mind in regards to how I approached stressors. I remember thinking about how all the things I stressed over were eventually resolved and gone, and all the stress had been for nothing. When I grokked this, the anxiety just went away.
As for OCD, I had some of the typical symptoms, like hand washing and checking, but the worst issue I had was intrusive thoughts of a blasphemous and hostile content. Ten years from when I first started having this issue, I became so sick and tired of the whole thing to the point that I had what I referred to thereafter as a nervous breakdown. I was tired of what I perceived as endless stupidity, and I just wanted it to be over. I made a massive effort to just block out all the evil thoughts and repress them. Previously, I would have been careful to remember a trigger thought so that I could neutralize it or “cancel it out” it with a proper ritual, but at this point I was just so focused on forgetting it that I couldn’t even perform the compulsion if I wanted to because I couldn’t remember what it was about. And I kept doing this hardcore. In about 1-3 months, everything just stopped. All of a sudden. I got that feeling you get when you’re in the room with someone, and then they leave and you’re left by yourself. I didn’t know at that time that my problem was demons. The Bible says, “Resist the devil and he will flee from you.” However, I don’t know if all these demons left me, or if some went into hiding, because from that point I had a 6 year break, and a few months before I accepted Christ as my savior, the torment came back.
I also had an issue with what I can describe very succinctly as asocial behavior. Given the opportunity, a psychologist or a psychiatrist probably would have diagnosed me as an aspie or a schizoid or whatnot, but all I can say is that this issue was resolved when a family member put pressure on me to be more open, to get a life, and I also took the focus off of myself (which interestingly enough, is usually the opposite of what psychology promotes).
First Job in Psychology
My first job in psychology was in corrections. The job of the mental health field in prison is a bit different than in a normal clinical setting. Prison is not a therapeutic environment, and perhaps the primary duty of psych here could be described as not to heal patients but rather to apply bandages (as one of my former colleagues put it), to keep them alive and chugging along. Actually, you could argue that point about mental health in general when it comes to severe cases, because “curing” isn’t really in the vocabulary of the mental health field.
I worked in a women’s prison and also a mostly men’s prison with a section reserved for a women’s psych ward. I worked with in total about 8 psychiatrists and psychiatric nurse practitioners. I knew 4 psych nurses, 6 psych techs, and there were many psychologists and social workers. They tended to come and go. I counted up to 22 in my memory. The lead psychologist position at the women’s prison was especially prone to a lot of turnover. Apparently worries about their license was a big factor. I used to joke in my mind at the time that the lead psychologist position was a bit like the defense against dark arts position in Harry Potter.
There was this one psychiatric nurse practitioner who was very intelligent and knowledgeable in his field, and I would pick his brain often, because remember, I was on the lookout for knowledge, to understand how the human mind works and what fixes people.
Diagnoses, Prognoses, and So Forth…
This psychiatric NP had a very pessimistic view from his experience, and I don’t think he was alone in this. I think this attitude is pretty standard for psychiatry. Less so for psychology; psychology is more optimistic.
We would get into a lot of conversations about diagnoses. He shared his clinical observations, like the differences between bipolar disorder and borderline personality disorder. He told me that borderline personality is usually misdiagnosed as bipolar. Borderlines, apparently, are desperate to get help, they want to try different psych meds, nothing ever works long term to make them get better, not even the much-touted dialectical behavioral therapy, and some would eventually isolate themselves so they don’t have to deal with the ups and downs of relationships anymore.
Bipolars, unlike borderlines, don’t want help, don’t want meds unless they’re in the depressive phase, and their condition worsens over time, resulting in cognitive deficits like attention problems. Schizophrenics – the real deal, as opposed to those with substance-induced psychosis, and yes, there is a difference – they tend to smoke; they often get charged with trespassing because they are prone to wandering around; and they usually have these vacant-looking eyes; and they tend to be strange and to do strange things that make no sense to others. At the prison, there was a patient that stashed used sanitary pads. Another one talked to insects and fairies. One had a child that was born with a severe birth defect affecting the legs, and she said she had wanted to chop off one of her own legs and offer it to the child. Like bipolars, they experience cognitive deterioration over time. Schizophrenics tend to pretty much waste their lives away living homeless or pretty much removed from society.
So, yes, those were some of his observations. Does it sound hopeless? Psychiatry tends to put forth this hopeless view that the patient will never recover but will always have to be on some kind of drug in order to maintain a measure of normalcy, and one could conclude that perhaps this is a reflection of the effectiveness (or lack thereof) of psychiatry. Interestingly, this psych NP would make a point of telling his patients that the medications don’t work as well as people think they do.
The therapists spent a great deal of their time with watches. Inmates that decompensated, that became violent or wanted to hurt themselves, were placed in an area called “watch cells,” where they were, quite literally, watched, sometimes continuously by security, and they were frequently checked upon by psych until they were deemed stable enough to be gradually stepped down until they were released to return to their usual housing. They were given a velcroed blanket to wear and had access to limited objects that they could use to hurt themselves. How well the watches worked for the purpose intended of preventing deaths is iffy at best. I knew of two hangings while I was working at the women’s prison, and neither gave any of the classic warning signs, therefore the deed was done before they could even be placed on watch.
The women’s maximum security yard had the bulk of borderline and antisocial personality diagnoses, and I remember how the therapy team used to get frustrated with them. (Quick FYI: when lay people use the term “antisocial,” they usually mean a person who avoids social interaction, but when psych people use it, it’s in reference to antisocial personality disorder, which is sociopathy. It’s a poorly-picked label, in my opinion, especially because some antisocials are very sociable.) So anyway, the borderlines created the bulk of issues for psych, especially because of self mutilation and self-harm threats. The prison allowed the inmates to have razors for shaving, apparently because it was considered inhumane for them to be deprived of a grooming tool. Go figure, when they could simply have provided them with sugaring kits that wouldn’t have created so many problems for psych. The razors allowed for cutters to self-mutilate, and there was a fair amount of that going on. I remember this one inmate whose forearm was so scarred from cutting, it looked no longer like human skin but rather like embossed leather.
Now, people who use psych services may be aware that the same person can get an entirely different diagnosis from a different provider. I saw this happening within the inmate population. According to my psych NP colleague, the reason for this tends to be incompetence on the part of some providers. He said that there is actually a lot of incompetence in psychiatry and after completing medical school, the lowest scoring medical students go into psychiatry for their residency. Apparently, in nursing it’s the other way around, with the top nurses becoming psychiatric NPs later on in their career. He said that a lot of providers do not do things by the book and they fail to dig into their patients’ history. They can also lack understanding of the lifestyles of their patients. For example, a psychiatrist from a middle class family who grew up sheltered might not even know to explore some of the life style factors of a patient who grew up poor and street-wise.
And I observed what he was saying playing out in reality. The psychiatrist who worked on the max security yard was very fond of the schizoaffective disorder diagnosis, and she was handing it out to drug addicts, to borderlines – patients who didn’t fit the criteria for these diagnoses. I will add that patients don’t always fit neatly into the categories created by psych. That said, if the psych field is good at anything, it’s describing clusters of symptoms and categorizing them. And you’ll find people that really do fit neatly into one or more of these categories. Psych, however, does tend to disregard and under-investigate the medical side of things. I myself observed that a number of patients with “bipolar disorder” also had a medical diagnosis of thyroid disorder on their chart – and there is a level of overlap between the symptoms of bipolar and thyroid disorders. Now, if these patients had had their thyroid issues properly treated, would the so-called bipolar symptoms have gone away? It’s possible. There is precedent of this happening. Having patients be tested for medical disorders was not standard practice; I just didn’t see it normally done.
The issue with disregarding medical can have serious, even potentially fatal consequences, and a close call of this nature happened while I was working at the women’s prison. I can share a glaring example of psychiatric incompetence. There was a woman in her early 30s who suddenly went psychotic. She lived on the max security yard, and her psychiatrist (the one with the affinity for the schizoaffective disorder diagnosis) just kept pumping her with more and more Haldol (which is an antipsychotic). Luckily, my psych NP colleague got involved in her case, and as a nurse practitioner he had a background in medical, so he realized this wasn’t schizoaffective disorder or schizophrenia or whatever her regular psychiatrist was insisting it was but rather a medical issue, and he advised she be taken in an ambulance to the hospital. He told them, either take her out of here in an ambulance or she’s going to be leaving in a body bag. It turned out she had gone septic from a urinary tract infection, which caused her to become psychotic, and if it hadn’t been for him, she would have died.
Imposter Syndrome
One thing I took away from my experience working in the mental health field is a feeling of imposter syndrome. I felt inadequacy to handle tough situations in a way reflective of superior knowledge of the human psyche that my field was supposed to provide, and I also felt inadequacy to effect much change in patients. I doubt I was the only one experiencing this. I suspect other psych workers may have experienced similar doubts. And I think this went both ways; I think the patients felt that the psych team wasn’t too helpful at times. One of the psych techs revealed that an inmate told her that she was useless. An inmate told me that her therapist just discussed fluffy stuff, like which Disney princess would she be. The therapists themselves expressed their frustrations at team meetings over the borderlines and sociopaths on the max security yard, and this frustration obviously stemmed from a feeling that they were unable to influence them for the better.
One thing that frustrated me was when I tried to run a psych education group, I observed not much interest and even some push back from the inmates. Generally, they didn’t really seem interested to learn about mental health, to gain information, which is completely opposite to my nature. But maybe I just didn’t a good enough job to grab their attention, because I was at a stage where I was trying to figure out things for myself. I do remember some more interest when I shared some Scripture-based material, but that didn’t go far because the psych leads shut it down.
As I described earlier, I had the opportunity to work with a decent number of psych professionals and some of these, despite their education and career experience, clearly dealt with unresolved issues. I knew a psychologist who was so filled with anxiety, her eyes were perpetually big like a deer in headlights, and she was frequently on edge. A psychiatric nurse who was convinced she was allergic to light. She would cover herself up with this big hat when she was going outside; she stayed in an office with no windows; and she reportedly lived (with her adoptive children) in a home where the blinds were kept shut. Another psychiatric nurse boasted about being a psychopath. I don’t know how serious she was, but who knows. A psychiatric provider used to drink and drive, concealing his alcohol in a large soft drink cup. Another psych provider openly disliked women in the workplace. I also knew a psychologist who apparently broke up her family to run off with a female prison guard.
I too had unresolved issues. The OCD was gone or dormant for about half the time I worked in prison. However, I experienced periodic episodes of depression that I had since I was a teenager. There was a growing gluttony issue, and I also had trouble getting over a breakup.
Now, I don’t think it’s a problem in and of itself to go into a field with issues relevant to the field. If anything, that would arguably make the person more relatable and more knowledgeable on the subject matter due to having first hand experience themselves – so long as they are actually able to fix themselves with what they have learned in said field. But if they are still struggling and their education didn’t provide the key to fix their problems, then what exactly qualifies them to help others? Does, say, an expensive psychologist with an addiction really have more to offer than just a random person on the internet who actually got over an addiction? Is a degree that really didn’t do anything worth more than free advice?
I don’t have any counseling success stories to share from my time at prison. Doesn’t mean there weren’t; I just didn’t know of any. Regarding psych meds… I’ve seen two or three patients improve on them. I remember one was diagnosed with bipolar and the other with schizophrenia. The schizophrenic had done cage fighting on the outs, and she had this aura of malevolence that I could tell even frightened her psych provider. This did not go away on meds, by the way. But my psych NP colleague noted that the schizophrenics still continue to hear the voices on the meds; it’s just more bearable. True to what he had told me, the borderline patients generally were indeed constantly asking to up their meds or to try something else, usually due to anxiety or mood swings.
The most impressive complete 180 degree transformation I saw was a woman who was saved by Jesus. I remembered her from the max security yard. She was possibly the worst case – her thing was climbing on the toilet and diving off of it head first to hurt herself. She was basically nonfunctional, spending a good deal of her time in a watch cell. Eventually, they decided to transfer her to the psych ward for women, and when I later went to work there as well, she was a completely different woman, having become vibrant, lively, and passionate to share her testimony of how she had gotten saved. Praise Jesus! It seems that one night, while she was lying on her back, her arms and legs were suddenly moved into the position of a cross, and a voice asked her, “Are you ready?” She was just really on fire to share her testimony, and her passion was something that impresses me even to this day.
All this time, I’m still wanting to find that special knowledge that would unlock the reasons for why people have mental health troubles and how to fix them. I never did find this key in psychology, though I felt I came close one time. I found this one site by a person who was interested in psychology. He wrote numerous articles that prescribed a common-sense approach. I would describe him as more of a coach, though he did get a psych degree at some point. I was inspired and my interest in psychology was reinvigorated, as I believed the key must be rooted in common sense – and a lot of what psychologists have to offer that will actually work is good old common sense and life experience, things that people you don’t have to pay will give you. I did want to make psychology work, to uncover value in it, because I still wanted to make a career of this field, and I didn’t want to make a career of something that is useless.
His information later helped me get over the breakup I mentioned earlier, when I actually made the effort to apply it. Good advice can be easy to find for a number of problems, but the issue is: are you going to apply it? I think that’s why a lot of people finally fix themselves when they hit rock bottom – because that’s what it took for them to work up the motivation. People can get used to, if not comfortable, with misery and just not be motivated to make a change until it gets too bad to bear.
I Got My Answer: What Causes Mental Illness & How I Came to Know Christ > Psychology
I got saved in 2017. I had been doing years of intense internet research on the spiritual realm. Maybe a year after I got saved, I learned about deliverance. I finally got my answer as to the cause of mental illness: demons living in our flesh. Yes, there can be physical causes too, like the inmate who got psychotic due to sepsis, but why would medical problems be free of spiritual causes? I’ve heard of people being healed through deliverance.
God blessed me to come across Chris Lasala’s videos, and my mom was watching Derek Prince. I was inspired by deliverance and tried to do it myself. I think it was in 2020 that I started going hard-core with deliverance. I had trouble with depression, bad episodes that came and went since, as I mentioned before, I was a teenager. I had a gluttony issue; I am a foodie at heart, and I loved to eat out and eat a lot. I developed insane food-cravings to the point that it was actually getting tortuous. I remember every day feeling pushed, just pushed, to go out and buy a specific food item (which would vary), and usually I had to drive a ways to get it. My brother and I had a running joke at the time (and it wasn’t about me specifically; it was just a general thing) that when one of us would get hungry we would joke that the parasite is ringing the dinner bell. And strangely enough, that was not far from the truth in my case. There were literally demons inside me ringing the dinner bell.
I also had a strange compulsion to wander, which I later discovered on the web was due to a vagabond curse on me. (You can google it to discover what it’s about.) It made me very restless, and I would just go for long joy rides, with my head in the clouds, listening to pop or rock (secular music) and drinking coffee. This was my idea of a good time, and I would waste a lot of time, money, and of course there’s the wear-and-tear on the car.
I don’t remember exactly how long it took for each issue, but I will estimate that about 1-3 months per problem area of doing probably daily deliverance freed me from these problems – glory to Jesus! And I want to emphasize that this was mostly self-deliverance I was doing. Compare and contrast this with people’s experience with the mental health system, where they spend years upon years talking to therapists, maybe even having to go on a wait list first in order to even see the therapist, or taking psych drugs with terrible side effects – and there is no lasting change, only brief relief. I’ve heard of people having the experience of going to therapy for 10 years and nothing changed. When one lady told me that, I asked her, “Why do you keep going?” The OCD issue appears to be a strongman. It’s taking longer for me to be free, but I’ve made a lot of progress, thank God.
Addictions Clinic
After my stint at prison, I worked at an addictions clinic. It wasn’t until I made this move that I realized just what a disaster the mental health scene is. At prison, mental health was mostly just about keeping people alive; here, I soon realized that, rather than helping these people clean up their lives, this clinic and no doubt others like them are oftentimes facilitating degenerate lifestyles for the sake of profit.
Although the place is listed as a non-profit, it’s clear to me that the purpose of the higher-ups is mostly if not purely profit. I say this simply because of the way the place was set up. It was not set up to motivate clients to change their ways and get better; it was set up to retain them as clients and to generate income.
For one, clients were allowed to treat employees almost any way they wished short of committing a crime and to engage in outrageous behavior on the premises. Actually, sometimes clients did cross the criminal line; I’ve heard of one employee getting hit, and I don’t think that client was charged. We were not made comfortable to correct or reprimand the clients with confidence. I mean, you could try, but you would be taking a chance. They had this grievance system set up, and if we offended a client, it came at the risk of said client filing a grievance, which would very possibly go in the client’s favor, seeing as they are the cash cow for the company. I do remember one colleague who confronted bad behavior, and she was passed over for a promotion that she wanted.
Billing was also very emphasized. The clinic received federal funding, and we had income quotas, believe it or not, and we had to bill a certain amount to insurance every day to make the quota; it almost felt like being a salesperson. Everyday was a race to make the quota, and whoever didn’t make it for a streak would be talked to about it. We were instructed on how to bill the most casual encounters in order to make this quota. I remember one colleague, a 75 year old woman, who had not made the quota for a period and she apparently had been warned if she didn’t pick up production, she would be let go.
Let’s get into the clients.
I want to say that there were a number of clients that genuinely needed love and help. My interactions with those people were very rewarding. I can not say that for the others.
Pandering to Low Lives
I remember this one verbally-abusive woman who had spent 10 years of her life doing meth. She would often go into profane tirades against the clinical staff. Usually, what would set her off is if somebody misunderstood something she said. We were not supposed to hang up on her without warning her, and a guy who worked there would just set his headset aside and let her scream and scream until she quieted down. She had apparently lost multiple children to CPS, but that didn’t put her off getting into the position of making more, as a coworker interrupted her during a tryst when dropping by for a home visit. Now, the interesting thing is that the employees were given a boundary in working with her, in which nobody was just supposed to hang up on her without warning during her disgusting tirades, but no boundaries were enforced on her, though that is exactly what she needed to push her to change as a person. She wasn’t my client, but I’m pretty sure she was living in taxpayer subsidized housing, because I’m almost certain she didn’t work. Personally, I believe picking cabbages in the field would have done more for her character than this clinic ever did.
Another client was a drunk, who when I did an assessment on him, apparently tied his condition to not having been able to get over being humiliated back in school. Apparently, he had been tied naked to a flagpole by other students, and the tape had embedded into his skin and he had to go to the hospital. Yeah, that’s traumatic, but if they hadn’t awarded him SSI for “alcohol dependence disorder” (which they did), this guy would have been forced to make an effort at life and perhaps make something of himself and move on. As it was, he lived on the government’s dole while drinking himself into the hospital, once coming close to dying after getting a stomach ulcer – from his drinking. A man in his 40s, no career, no job at all, just boozing and trawling bars on the tax payer’s back. He once ended up in the psych ward at a hospital because apparently somebody had spiked his drink with some kind of hard drug. Basically, a man with no incentive, no motivation to change his course in life.
BTW, the average client at the clinic was in middle age or older, lots of them having destroyed their lives in their youth with vice and were now living with the consequences of their behavior – or as much consequences as the mental health industry and government charity allow.
There was this one female client in her late fifties or early 60s, I believe, who had lived off of SSI herself for 20 years on the basis of a diagnosis of depression. She had wanted to change her housing, and I noted how insistent and persistent she was to get help. This woman could definitely advocate for herself, and I remember joking to a colleague that she would make a good bill collector. So, why was she off the hook to work because of her depression? I observed that it wasn’t interfering with her ability to function. She even got a new boyfriend when she moved into her new apartment. I myself have worked with depression. If anything, one could argue that it’s good for people with depression to have something to get up for.
A truly vile client would lock himself in the bathroom to smoke fentanyl, and nobody was supposed to call the cops. BTW, he wasn’t the only one to do drugs on the premises. This made me so mad, especially because in order to get this job, I had to undergo an extensive background check and pee in a cup like a criminal to prove that I wasn’t on drugs – only to find out that there were such double standards! I was so mad that open criminals are allowed to access free federal money to support their lives whereas if I did what they do I wouldn’t be able to access a job where I actually would have to work in order to support myself. It’s a slap in the face.
One homeless client straight up admitted having no intention of quitting meth. He was snorting meth every day, and he said he likes the way it makes him feel. He was erroneously diagnosed with schizophrenia, and he was taking an Invega shot, obviously to help with the side effects of the meth. (Invega is an antipsychotic, by the way.) Obviously such people are just using the system for freebies and psych meds to treat the side effects of their drugs, like being unable to sleep. Now, if this clinic actually had the best interests of their clients in mind, they would have made drug testing mandatory. That is to say, if you fail the drug test, you can’t get any benefits – otherwise, there is no incentive to stop. I don’t think it’s fair to enforce drug tests on workers but not on government charity. I mean, you can argue against my position by bringing up the drug program in, say, Portugal, but if you actually look into it, it hasn’t cleaned up their drug problem. The addicts are merely being supported into perpetuity by the tax payers, and the taxes of the people are high. Is that ethical, to take money from taxpayers to support sin? You tell me.
Speaking of psychotic issues due to drug use, I found multiple instances of such clients who were diagnosed with schizophrenia, bipolar – diagnoses for which they were not qualified if their providers were doing things by the book. And they were, of course, on psych meds to relieve the symptoms of their ongoing drug use. Now, diagnoses of bipolar and schizophrenia are supposed to be ruled out if the patient’s symptoms are the direct result of drug use. Nevertheless, this problem with psych providers handing addicts diagnoses for which they do not qualify is rampant. Back in my prison job, I learned that psych providers will sometimes give patients the wrong diagnosis in order to qualify them for benefits that they wouldn’t get otherwise – now, doesn’t that sound unethical?
Another client was a meth addict who would fake – and everyone knew he was faking it – feeling like he wanted to end his life so he could go and spend time in the hospital, again on the tax payers’ back, while ignoring the subsidized housing that he had been provided. He was doing this constantly. Apparently, these psych wards cannot turn people away, no matter what, if they say the magic words.
I remember this diagnosed sociopath with multiple addiction issues; he was awarded temporary housing, and guess what was first thing he did when he went to his housing? He destroyed the room within four hours of getting the place. He punched holes in the walls, spray-painted the place, threw the furniture all over, and then vanished. Did they call law enforcement on him? Apparently not. He had an extensive criminal history, and yet he was on a voucher for subsidized housing.
The clinic had several vans for employees to use, and every so often somebody would steal the catalytic converters at night to sell, because apparently they contain platinum. We had an inkling who the culprit was (a particularly sociopathic client who once did a stand off with the clinical director in the lobby), but we couldn’t prove it due to not catching him red-handed. When I asked my boss why there was no video surveillance in the parking lot, she told me that they can’t have surveillance there because what if the clients decided to have sex there and got recorded?
One of the clients I caught abusing the cab system for personal trips. This guy volunteered at the snack bar, and it came out that he was stealing from the till, and apparently, no action was taken against him.
In numerous cases, these mental health diagnoses become excuses for bad behavior, and the recipients are being taught that in some situations they are above the law.
And the low lives abused this because they were aware that there were generally no consequences for them, other than possibly getting petitioned to go to the psych ward – which at least some of them didn’t find to be such a bad thing if they wanted to go there of their own free will. I guess for someone who is abusing street drugs, getting pumped up with psych meds is nothing to worry about. At least they’ll be able to sleep. Bottom line, the top hierarchy couldn’t care less about their employees, and it was in their interest to keep the cash cows comfortably living in sin, on the highway to hell, in order to line their pockets.
I would say that the average psych workers were codependent, like enabling family members. I admit I was not always much better than them in this regard. I didn’t buy into the humanistic mindset that is rampant in psychology that everyone is essentially good and you got to nurture them and show them unconditional positive regard so they can grow and all that. If you show a sociopath unconditional positive regard, he’ll take you for a fool and an easy target. That said, I didn’t call out as many clients as I should have. One of my clients, though, I called out on his sin, and I’m glad I did, because he kept at the drugs and then one day he literally dropped dead while walking with another client – so his blood is not on my hands for failing to rebuke him, thank God. I remember speaking to another client, too, about her sin, and I had discussions on Christian matters with another two clients.
There was this one woman who I didn’t tell off (and I should have), who did something wrong (I don’t remember what), and she looked at me and said with this smirk on her face “By the way, that was my bipolar.”
Most if not all of these clients that I discussed appeared to be able-bodied, and I suspect a number of them would be able to hold their behavioral issues in check if they were subjected to normal societal pressure and the need to earn an income.
Facilitating Delusion
This clinic would often invite guest speakers, usually reps from drug companies marketing the latest psych med innovation. This one time, they had this person over to talk about binders and where to find them. When I saw the invite, I was wondering if by “binders” they meant office supplies? However, when I arrived for the presentation, I beheld a delicate, petite woman who was obviously trying (very unsuccessfully) to look like a man. She informed the room where they can locate for their female-to-male transgender clients a device to compress the breasts to make their chests look more male-like, to help with the illusion.
When I had enough, I got up and walked out of the room. When my boss wanted to know why I wasn’t there, I told her I cannot partake of that. She seemed miffed but she didn’t try to pressure me or persecute me, so kudos to her for that, though the reason is probably not wanting to stir up legal issues. Afterward, I did imagine a way I could have handled things differently, that instead of walking out, what if I had instead asked the guest speaker that if I had a client who thought he was the pope, where can he get a good pope costume?
Now, the Diagnostic and Statistical Manual (or DSM) is a the hand book the mental health field uses to make their diagnoses, and it used to have a diagnosis for “transsexualism,” later called “gender identity disorder,” meaning in the past they did see this as problematic. They updated this to “gender dysphoria” in 2013, with the focus of the problem being switched from the sense of not being in the right body to the distress caused by this situation. However, they have still have retained the concept of a delusion, and if you look at the DSM-5-TR (which appears to be the latest version of the DSM), this is the definition you will get for a delusion: “fixed beliefs that are not amenable to change in light of conflicting evidence.”
So, why is the mental health field now facilitating something that by their own definition constitutes a delusion? Are they just saying that you can just pick and choose which fixed beliefs that don’t match reality are mentally sound and which ones are not? Well, they did use to have homosexuality down as a mental health disorder as well, but they took that out in 1974, apparently due to successful lobbying by the homosexuals. I guess to them mental health can be a matter of politics. Any logical person should immediately see the problem that is inherent. How confident would you be going to a medical doctor if they based their diagnoses on politics?
Incorporation of Eastern Religion and the Occult
The other thing they were doing at the clinic (and this was not just for the psych people, this was directed at the medical staff there as well) were these trainings on the computer, and these were mandatory. There were two trainings, if I remember right, in which they were teaching occult practices and ideas as methods of relaxation. I am talking about yoga, I’m talking about mindfulness, and I think there was something else that is slipping my memory. Yoga, a Hindu religious ritual, is prescribed for relaxation! I refused to complete these trainings, citing my religious concerns, and they acquiesced.
Psychology has actually adapted aspects of the occult and eastern religion under the guise of science since its inception. It goes back to Freud, who used hypnosis on his patients even though he was an atheist. I guess you can try to avoid religion but may just end up in some kind of religion anyway. Carl Jung, by the way, was just immersed in the occult; he consulted a familiar spirit for ideas, he conducted seances, and so on. So, you could argue that psychology is not completely secular, though they may argue that they strip the religious connotations out of the practices that they adapt – if that’s even really possible. Can you say for sure that the spirit realm respects that you are doing what was originally supposed to be a ritual, but you are not doing it for spiritual purposes? I mean, if you took some salt, sprinkled it in a circle, then sat in the center and chanted an incantation for the “relaxation,” do you think the demons would say, “Nah, she doesn’t mean it; let’s not show up.” You tell me. What I will say is that there are reports of people experiencing psychosis from doing eastern style meditation, which tells me they got demonized. Here’s one from an atheist.
He wasn’t doing it to practice a religion, obviously. I myself experienced a bizarre demonic experience when I tried doing yoga years ago before I accepted Christ, and I was definitely not trying to be a Hindu.
I didn’t do yoga because of psychology, but in the past, I actually was duped into the occult directly because of psychology. I did do mindfulness when I was in college without even knowing what I was doing. I just realized this recently, when I looked up to see what exactly mindfulness is. One of my psych professors taught the class to do mindfulness meditation (he never did say what it was; even if he did, I just don’t remember and it wouldn’t have meant anything to me anyway), and he said this was supposed to bring better rest than sleeping, which is clearly balderdash. At the time, I had trouble sleeping, so I would use this at night to try to go to sleep. It wasn’t something I grew fond of. It was very dull, I don’t think it worked that well for the purpose I employed it, and I can’t think of any benefit that I got out of it. I probably picked up some demons. Nowadays, if I can’t sleep, I just stay up on the computer until I get sleepy.
Later on, after college, I got interested in hypnosis, and they were trying quite successfully to pass it off as science, talking about alpha waves and other such jargon. Deep under this deception, I got fascinated by the potential of hypnosis, and I even obtained a certification to be a hypnotherapist at one point (this was before I saved, before my job at the prison). Thankfully, I made little effort and progress into this endeavor, and when I learned this is a technique that witch doctors employ, I repented of my involvement in this practice.
Wake Up Call
I came to the conclusion, also due to my mother, that at my position at the addictions clinic, I was actually perpetuating an unethical, immoral situation, in which I was facilitating people to continue in wrong lifestyles. Willful addicts and freeloaders on society. Now, if everybody declined to work with these kinds of people at this kind of a clinic, there would be nobody to facilitate their degenerate lifestyles, and they would be forced to make an effort. The mental health field is actually making people comfortable in their sin and leading them to hell. These people don’t need psych meds to relieve the unpleasant side effects of their recreational drugs or some therapist to ask them like a broken record, “And how do you feel about that?” From my own experiences with mental health, I can attest that they need a call to repentance, they need prayer, and they need deliverance.
My greatest wake up call about psychology was when I came across the teachings of Dave Hunt. He made some fantastic exposes on the field of psychology. Driving to and from work, I was listening to radio recordings of his site, The Berean Call, and learned shocking new things about the history of psychology and its atheistic origins.
Here are 3 problems with psychology:
1. To quote Dave Hunt, “mental health professionals can’t fix themselves and they don’t have the answers” – I saw this for myself when I was working at prison. Some of the workers there were just as messed up, if not more so, than the patients. I, too, was not where I should have been, though it’s possible I had more success in resolving personal mental health issues than the average worker — I don’t know.
2. As Dave Hunt argued, psychology operates under a mantel of science, but it is not science. Many of these psych therapies are not scientifically tested and could be better described as philosophies or even religion, especially considering that psychology has borrowed pagan and occult ideas and practices. Even those therapies that have been tested don’t work as well as you would think – and I will get into that. As for psych meds, the psych NP I knew back in prison told me that finding the right medication is like throwing darts at a board and seeing what will stick.
3. And the third issue is that the mental health field facilitates sin – I think I’ve already given enough examples.
Psychology’s Damning Research
Interestingly enough, psychology itself has done the research that shows that it’s a fraud, that the emperor doesn’t have clothes. They themselves have demonstrated scientifically that their theories tend to be bunk and on average they are not helping people, but this is swept under the rug so business can go onward. In regards to what works to treat addictions, here is what psychology research has to say:
Psychotherapy as a treatment for alcoholism… appears to be quite ineffective. Thus, Gerard, Saenger, and Wile (1962) studied the long term effectiveness of clinical services for alcoholic patients. The authors chose a random sample of 400 patients from state-supported alcoholism clinics. The patients were randomly interviewed at either two, five, or eight years following intake. Of the 299 patients reached in the follow-up, only 18 percent remained abstinent for at least one year during this follow-up period [that’s less than 1 in 5]. Of the others, 41 per cent were unchanged, while 10 percent had deteriorated to the point where they were institutionalized, and an additional 17 percent were dead. Quite significantly, among the 18 percent who actually remained abstinent for a least a year, more than half continued to manifest gross overt symptoms of psychologic impairment. Of this same 18 percent, only 10 percent sustained their improvement independently, while the rest relied on Alcoholics Anonymous, etc. Quite surprisingly, the drinker who finally abstains rarely quits drinking during psychotherapy. The most common reasons given for abstinence were fear of death or severe liver damage or arrest. Those few who were relatively sustained in their abstinence most commonly gave as their reason, “people like me better sober.”
– Robert R. Carkhuff, Psychologist (1967). Toward Effective Counseling and Psychotherapy (2017 edition)
So again, we’re returning to the issue of motivation. Drugs like alcohol feel good, and it’s hard to let go of something that feels good. Having a friendly conversation with some therapist isn’t going to motivate someone quite the same as fear of dying, sickness, or loss of relationships. I experienced this myself with my past coffee addiction that I quit before I worked at this clinic. I kept going at it until I had this scary dream that basically warned me I would die, and then I stopped cold turkey.
In contrast to the soft soap, permissive attitude the clinic I worked at took toward its addict clients, here is another study that shows what really works. This quote comes from Manufacturing Victims, by Dr. Tana Dineen, a psychologist who calls out her former field of practice and who quit practicing psychology because it seems her conscience would no longer allow her to be in this field with all the ethical problems it has.
Ditman studied three groups of alcoholics who had been arrested and charged with alcohol-related offenses. The court had assigned these individuals to AA, an alcoholism clinic, or a non-treatment control group. A follow-up found that 44 percent of the control group were not re-arrested, compared to 31 percent of the AA group and 32 percent of those treated in a clinic; those that received treatment did worse than the untreated. “Not one study,” Peele asserts, “has ever found AA or its derivatives to be superior to any other approach, or even to be better than not receiving any help at all. Every comparative study of standard treatment programs versus legal proceedings for drunk drivers finds that those who received ordinary judicial sanctions had fewer subsequent accidents and were arrested less.”
– Tana Dineen, Psychologist (1996). Manufacturing Victims (2007 ed.), p. 55
To stop bad behavior, fines and jail work better than unconditional positive regard, coping skills, and being asked about your childhood trauma – who would have guessed?
Speaking about bad behavior, remember the client who blamed her bad behavior on a diagnosis of bipolar? This quote from Dr. Tana Dineen perfectly explains why she did that:
When once people were ashamed of being diagnosed, many are now eager and willing, provided that the label (1) explains and justifies their problems and behaviors, leaving them with little or no sense of guilt or responsibility, and (2) is socially acceptable, making them feel special and understood without feeling stigmatized.
– Tana Dineen, Psychologist (1996). Manufacturing Victims (2007 ed.), page 75
In regards to psychiatric diagnoses making people feel special… I remember reading this comment chain in which a bunch of boys were basically patting each other on the back and boasting of their “neurodivergent superpowers.” Apparently, their neurodivergent superpowers consisted of – get this – being jerks to their teachers. Teachers are apparently in the same boat as psych workers in clinics – actually probably worse – essentially close to helpless to do anything about bullies. I left a comment to the effect that in the past when teachers could use corporeal punishment, their neurodivergence would have been cured pretty fast. No one responded last I checked.
So, the interesting thing about the mental health field is they have the research to show what works and what doesn’t. And yes, I’m aware that most psych workers are unfortunately unaware of this damning research I mentioned. However, this doesn’t matter as much as you would think, and I’ll explain why.
From the outside, we can’t really tell a lot of what’s going on inside a person. Objectively speaking, a lot of what is called mental illness can be observed to be behaviors. And people instinctively know what to do to quash behaviors that they don’t like.
But when I mentioned punishment, one of my colleagues turned on me. “No, no punishment!” See, the ironic thing about that is that she then had no problem putting in a bad word about me to the boss in order to interfere with my employment and therefore punish me for my opinion (she didn’t succeed, thank God). Noo, don’t punish the sociopathic clients – punish the one who wants to straighten them out. But my point is: they know what works to stop behaviors that they don’t like. When one of my coworkers mouthed off her boss, she wasn’t coddled, she wasn’t asked about her childhood trauma; she was fired. When another employee reportedly failed a drug test, it seems his boss didn’t tell him “Oh, poor you, you have a disease; I understand,” because we never did see that guy again. But when the foul mouthed client, for example, screamed obscenities at the staff, she was given no warning or rebuke that I know of, and instead, the staff were given a boundary in working with her. You would think that the higher ups would know that by letting bad behavior go unpunished, they are in fact rewarding and reinforcing that behavior. Wouldn’t they know a thing or two about operant conditioning, being in the psych field and all? I think they do, as evidenced by big mouth = no job, failed drug test = no job. And, oh, subpar performance = at risk of losing job. Problem is, in regards to clients such as the foul mouthed one, if she’s booted, the income is lost. And if she’s subjected to a system of punishment and reward, and by some stretch of the imagination submits to it until she learns self-control, she’s eventually going to graduate and make it on her own – and then income, again, is lost. Anyway, Dr. Tana Dineen touches on the mental health industry’s drive for continued income in her book Manufacturing Victims, and I do recommend her book.
In regards to lower level psych employees who don’t get a say in how things are run, I’m pretty sure many if not most tolerate and therefore perpetuate bad behavior simply because they don’t want to risk getting fired – which again, comes back to income. I was in this position as well, though I did step out of my comfort zone and draw a line at times. Of course, when psych workers are hobbled like this, it follows that treatment effectiveness is sacrificed as a result.
Another problem is unfortunately that it’s possible that many if not most psych people have bought into the falsehood that the mental health industry teaches, that mental illness is due to defective brains, chemical imbalances, and so forth. I do remember overhearing a colleague complaining to a clinical coordinator about a nasty client (really, some of these clients were truly abusive, and the employees were normally not supported at all. I mean, this is pretty common in customer service, where profit and sales is the primary objective, but you would think in mental health, where personal improvement of clients should be the priority, things would be different. Really shows where their interests lie). Anyway the CC was just going, “Oh, they’re mentally ill.” Well, what’s the difference between a common jerk or someone diagnosed with intermittent explosive disorder? It turns out that the mental health industry can’t tell you.
The incredible recent advances in neuroscience, molecular biology, and brain imaging that have taught us so much about normal brain functioning are still not relevant to the clinical practicalities of everyday psychiatric diagnosis. The clearest evidence supporting this disappointing fact is that not even 1 biological test is ready for inclusion in the criteria sets for DSM-V. Fortunately, the NIMH is now embarked on a fascinating effort to effect the real paradigm shift of basing diagnosis on biological findings. Unfortunately, this is years (if not decades) from fruition.
– Allen Frances, Psychologist (2009, June 27). “A Warning Sign on the Road to DSM-V: Beware of Its Unintended Consequences.” Psychiatric Times, Vol. 26, Issue 8.
So, what he’s saying is all the cool stuff they learned about the brain can’t be used to diagnose mental illness.
It has been years since this quote was made in 2009, over a decade in fact. Let’s jump forward to 2022, shall we? BTW, Allen Frances was chair for the task force during the fourth revision of the DSM – so he’s not just some random psych worker. But anyway, let’s go to the next one.
In 1990 President George Bush announced that “a new era of discovery” was “dawning in brain research.” Over the next several decades the U.S. government poured billions of dollars into science that promised to revolutionize our understanding of psychiatric disorders, from depression and bipolar disorder to schizophrenia. Scientists imagined that mental illnesses in the future might be diagnosed with genetic tests, a simple blood draw, or perhaps a scan of your brain. New pharmaceuticals would target specific neurochemical imbalances, resulting in more effective treatments. … The reality of psychiatric practice is far less glamorous than the visions of its future that I grew up with. Thirty years later we still have no biological tests for psychiatric disorders, and none is in the pipeline.
– Marcos Ramos, Psychiatrist (2022, May 17). Mental Illness Is Not in Your Head. The Boston Review.
Welp for the psych industry.
And here’s a director of research at the American Psychiatric Association. He says he doesn’t know what causes any mental disorder.
I’m the director of research at the American Psychiatric Association. We don’t know the etiology of really any of the mental disorders at the present time.
– Darrel Regier, Psychiatrist (2008, Feb. 27). The Diagnostic and Statistical Manual of Mental Disorders (DSM). [Video]. Youtube.
Today, science has the necessary technology to determine whether or not chemical imbalances exist, but none have been found. It is this fact that has prompted the present (2014) director of the NIMH, Thomas Insel, to state that “earlier notions of mental disorders as chemical imbalances or social constructs are beginning to look antiquated.” Also, William Whirsing, M.D., professor of psychiatry at UCLA, stated to a room full of psychiatrists that “We have been misleading the public about the chemical imbalance model for 40 years.” Finally, ex-director of the NIMH, Steve Hyman, upon summarizing over 40 years of research pertaining to the effects of antipsychotic drugs, reported that the use of the drugs actually creates, rather than corrects, a biochemical imbalance within the brain and in fact works similar to drugs of choice or street drugs.
– Ty C. Colbert, Psychologist (2017). The Four False Pillars of Biopsychiatry.
That psych NP from prison that I mentioned so many times would get kind of riled up when patients brought up self-medicating on street drugs; he didn’t think it was a valid thing, but the people who claim to do so actually have a point. If psych meds work like street drugs, then the only real difference is that psych meds are pharmaceutically pure and you’re not ingesting gasoline or some other nasty adulterant — and I guess another difference is that the dosage is not supposed to be big enough to get you intoxicated, though I have seen enough over-medicated psych patients looking like zombies.
Ok, so some are fessing up as to how the mental health field has deceived people about the biological basis of mental illness. However, does this mean that psych meds don’t work? Let’s see what Psychologist Irving Kirsch and his graduate student Guy Sapirstein had to share:
So Irving and Guy started to compare the results for antidepressants… in every study that had ever been published. To find out the chemical effects of the drug, you do two things. First, you subtract all the people who would have just gotten better anyway. Then you subtract all the people who got better when they were given a sugar pill. What’s left is the real effect of the drug. But when they added up the figures from all the publicly available scientific studies on antidepressants, what they found baffled them. The numbers showed that 25 percent of the effects of antidepressants were due to natural recovery, 50 percent were due to the story you had been told about them, and only 25 percent to the actual chemicals.
– Hari, Johann, Journalist (2018). Lost Connections.
So it looks like they did a meta analysis on all the studies on antidepressants. The result was that only 25 percent of the antidepressants’ effect was due to the chemicals themselves (so just a quarter of the total effect) – and the majority was placebo effect and some was simply natural recovery.
The mental health field admits that they have been deceptive about the biological model of mental illness – and some of this is coming from the mouths of big wigs, not just small guys with bad consciences. Now, let’s see what they have to say about how well psychotherapy works.
The field of counseling and psychotherapy has for years presented the puzzling spectacle of unabating enthusiasm for forms of treatment whose effectiveness could not be objectively demonstrated. With few exceptions, statistical studies have consistently failed to show that any form of psychotherapy is followed by significantly more improvement than would be caused by the mere passage of an equivalent period of time.
– Jerome David Frank, Psychiatrist in Truax, C.B. & Carkhuff, R. (1976). Toward Effective Counseling and Psychotherapy: Training and Practice, (2017 edition).
So, you could have been going to a therapist for years, and after some time, you feel better, but you don’t realize that you could have been using that time to do things that you actually wanted to do and would have ended up feeling just as good, plus your pocketbook would be thicker.
In a review of therapy factors that account for significant client progress, Lambert calculated the percent of improvement that could be attributed to each of several variables… He found that “spontaneous remission” (improvement of the problem by itself without any treatment) accounted for 40%, an additional 15% of the change resulted from placebo effects (which he referred to as “expectancy controls”, that is that the patient expected to get better no matter what was done,) while a further 30% improved as the result of common factors in the relationship such as trust, empathy, insight and warmth. Only 15% of the overall improvement could be attributed to any specific psychological intervention or technique. Based on these findings one could conclude that 85% of clients would improve with the help of a good friend and 40% without even that.
– Tana Dineen, Psychologist (1998). Psychotherapy: snake oil of the 90’s. Skeptic Magazine 6(3)
Ok, so this guy found out that most improvement was due to people just naturally getting better, 30% improved due to what is called the therapeutic alliance (a fancy term for what essentially is perceived love), and tied for 15% was the placebo effect and the specific technique used. The conclusion is that 85% of the clients would improve with the help of a good friend and 40% without even that.
If the type, length and intensity of therapy generally have no significant effect on clients’ improvement, one would hope that at least the therapist’s training does. To examine this, Strupp and Hadley randomly assigned thirty clients with neurotic depression or anxiety reactions to either university professors who had no background in psychology or psychotherapy, or to professionally trained and accredited psychologists. They found that the professionals were no more effective than the untrained professors, as assessed on a number of measures of clients’ functioning.
– Tana Dineen, Psychologist (1996). Manufacturing Victims (2007 ed.), page 54
And now some may counter: well, something’s wrong with the research. You’re cherry-picking the research. And to that I will answer: the ultimate test of any research is to match it up against what’s happening in the world, what you can observe in the world. Despite what some may argue, there is more access to mental health services than there has ever been before, the stigma of having a mental health diagnosis has decreased (not increased), and the use of mental health services has gone up over time, not down. Therefore, you would expect that societal mental health would have improved, if these so-called experts knew what they were doing. So, let’s see what’s actually happening with mental health in the news, shall we?

Well, look at that: the hotlines they keep promoting do nothing to stem the problem. In fact, it looks like it’s getting worse.
Good question.
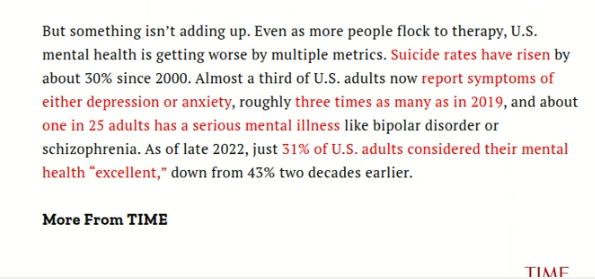
Not looking good for psych.
Two possible explanations come to mind: the supply is not keeping up with the demand or… psychology is not only ineffective but actively causing harm.
Check out this graph… wow.
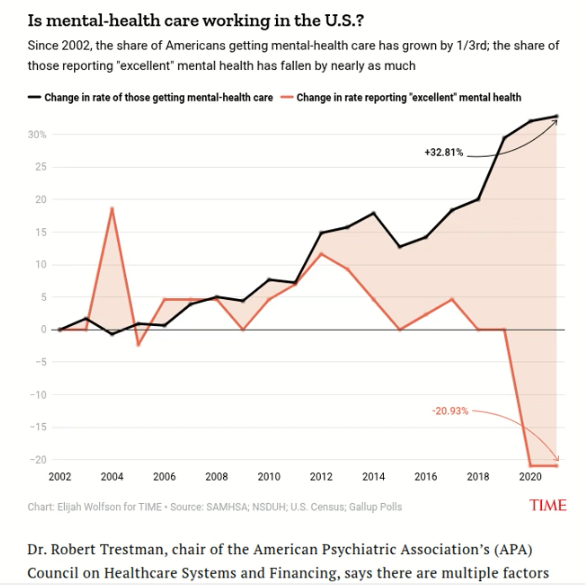
It’s pretty clearly showing that greater use of mental health services coincides with worsening mental health. This brings to mind a couple of researchers from the 60’s, Truax and Carkhuff, who concluded that on the average, psychotherapy may be harmful as often as it is helpful, with an average effect comparable to receiving no help.
However, looking at this chart, we see a much bleaker picture than those two researchers concluded. The nation-wide data shows an average effect suggesting that active harm is being done. Or maybe a large portion of the people getting mental health care are simply stuck on a wait list going crazy – I don’t know. We do know that natural recovery is a reality. The chart does say “getting,” not “seeking,” so I will assume these people are receiving the mental health care. You know, if the data for cholesterol medication showed that the more people took it, the higher their cholesterol got, wouldn’t you think there’s a serious problem with the medicine? Look at this:
Bingo.
Oh, so these older adults who are less likely to use mental health services but rather go to church are not doing worse, just the young people who as a whole are increasingly disconnected from Christianity.
From the article: “Twice as many young adults spent half or more of their days in poor mental health in 2018–20 compared to 1993–99. Nearly all of the increase occurred before the COVID-19 pandemic began in 2020.”
So you can’t blame it on that.
On to the next article.
Hmm.
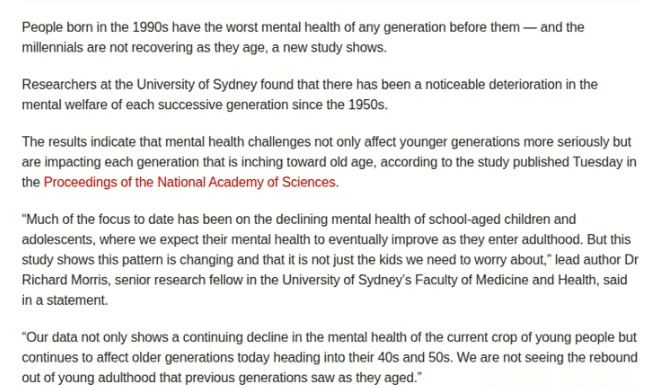
From the article: “Researchers at the University of Sydney found that there has been a noticeable deterioration in the mental welfare of each successive generation since the 1950s.”
The 50’s, huh. That was when counseling started to get popular. Is that a coincidence?
Also from the article: “Our data not only shows a continuing decline in the mental health of the current crop of young people but continues to affect older generations today heading into their 40s and 50s. We are not seeing the rebound out of young adulthood that previous generations saw as they aged.”
I guess that’s just what happens when you rely on the theories of dead philosophers instead of the Word of our live King.
Conclusion: Christ Trumps Psychology & the Mental Health Industry PERIOD
So, after studying psychology in college and working in this field for several years and doing years of searching on my own time, I came to the conclusion that psychology is nothing more than an inferior, pseudo-secular substitute for what Christianity has been offering all along to heal the soul.
I say pseudo-secular because even though it’s supposed to be a secular alternative to religious counseling in general, that is debatable, because as I mentioned earlier, they do incorporate religion, and they have derived ideas from the occult. And some of their theories essentially offer a framework for living one’s life and could be in their own right labeled a religion.
I actually repented to God of having gone against my mother’s wish for me to have studied nursing rather than psychology, and I know He was pleased with me for having repented. If I had gone into nursing instead, I think my life would have been so much more rewarding; I could have done travel nursing, seen a lot more of the world, had more fun, likely more stress, but definitely more money.
The psych field rejects the power of God in favor of human potential. And that doesn’t work. There are so many people sharing their testimonies online of being cured from mental illness through deliverance. (I have featured a number of these here). So, when demonic oppression rather than a biochemical imbalance is the cause of mental illness for so many people, as I discovered to be my case as well, then how can this industry fix people using secular methods or even the occult disguised as science? I could liken some of my past struggles with mental health to falling down a well and good advice that I came across to a rope being lowered down. But the rope is about five feet too short. I couldn’t jump five feet on my own; I needed supernatural assistance because I had a supernatural problem.
Jesus is the real healer, not mental health professionals. I’ll leave you with some excellent quotes I came across from Dave Hunt. Take care, and be blessed.
More articles: