“The Psych Meds Are Not Working” – This is Why (If You Did Drugs)
Imagine a beautiful old house. Now, imagine you bought this house. It is winter, and you want some heating. There is no central heating system, and the fireplace has been bricked over. So, you go buy a radiator and plug it in. The radiator will not turn on, and the house remains cold. You try plugging it into other outlets, and it still doesn’t work.
At first, you suspect that your brand new radiator is defective. It is a long trip to town, so rather than returning it to the store right away, you take it over to your handyman neighbor to see if he can find the problem. He plugs it in at his house and (surprise!) it works just fine.
The problem was not the radiator; it was your house’s bad outlets.
People with a history of drug use can experience a similar frustrating scenario if they seek relief from mental health symptoms using psychiatric medication.
They might get on medications that they know worked well for other people. However, it doesn’t do much for them. They have to keep asking their psychiatric providers to up the dosage or to switch them to something else. The cycle of trying new medications and increasing doses can go on for years. And yet, nothing will bring satisfaction.
In my earliest position in mental health, I remember sitting with a psychiatric nurse practitioner as he diagnosed patients and saw returning patients for checkups. (For those who are not familiar with the term, a psychiatric nurse practitioner more or less performs the same duties as a psychiatrist.) Many of the patients had a history of substance abuse, and oftentimes they would report that the medications weren’t working and request an increase in dosage. I remember him painstakingly explaining to them that 1) psychiatric medications are not as effective as most people think they are and 2) the meds might not be able to work because of their history of drug abuse.
Here’s why.
Depending on the individual sensitivity of a given person’s brain tissue, the types of drugs abused, the adulterants in the drugs (which can range from dental anesthetics to solvent residues), and the duration of abuse, people with a history of drug use can have varying levels of brain injury. As my former colleague told his clients, the medications are less able to work simply because they don’t have where to plug into.
To provide a better picture of the problem, let’s start with a diagram of a neuron.
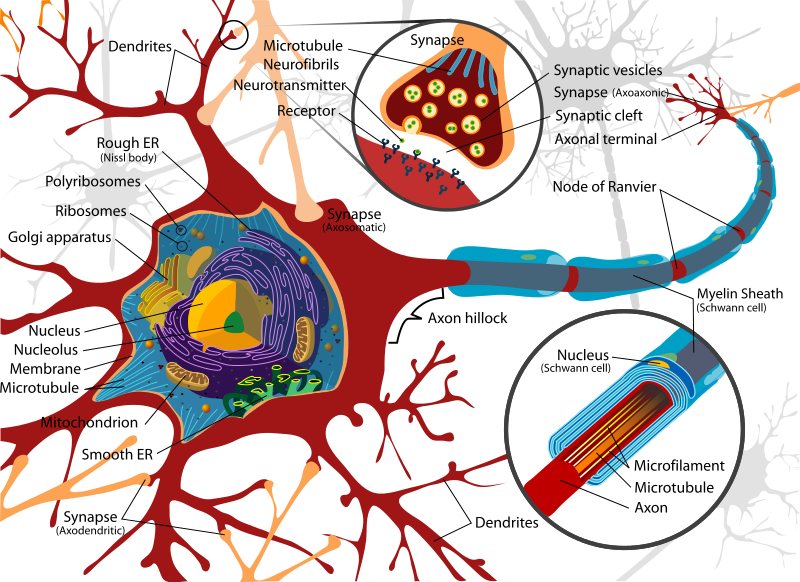
Let us direct our focus to the tiny channel between the neurons (indicated by the two smaller circles at the top of the image), called the “synapse.” This is where the communication between neurons takes place via neurotransmitters. In order for a neuron to pass a message along to another one, it releases neurotransmitters, which then plug into the specific receptors in the next neuron, sort of like pushing a button, in order to transmit the message. Depending on the type of neurotransmitter, the message could be “Get excited,” “Concentrate,” Feel calm,” etc. After stimulating the receptors on the other neuron, the neurotransmitters are reabsorbed, or taken back up, into the neuron that released them.
Consider a psychiatric medication like Paxil. Paxil is an SSRI,which stands for “selective serotonin reuptake inhibitor.” The way this medication is supposed to work is by plugging into the neuron that released the serotonin and not allowing it to reabsorb the serotonin. The serotonin then accumulates in the synapse and keeps stimulating the other neuron. Here is a quick video to provide a more visual overview.
With a damaged neuron, there are fewer to no receptor sites for both neurotransmitters and Paxil (or another psych med) to plug into. Obviously, a person missing a percentage of their serotonin receptors will see much less benefit from an SSRI than someone whose receptors are all intact.
Here is an example of changes in the brain with drug use (cocaine). Cocaine is a drug that produces a high by revving up dopamine activity in the brain. Below, observe the PET scan of a person who never used cocaine (left) as compared with a cocaine user (center). The picture on the right is a scan of the cocaine user’s brain after 4 months of abstinence.
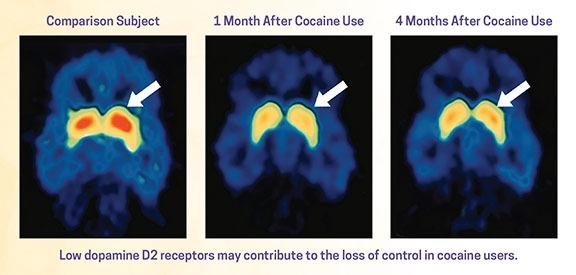
The red areas indicated by the arrows show the dopamine receptor (D2) activity in the brains, which is clearly higher in the non-cocaine user’s brain but nearly absent in the user’s brain. After four months of abstinence, the brain of the person who used cocaine has some restored dopamine receptor activity; however, it has not caught up with the non-user’s brain. On a slightly off-topic note, after looking at this it makes sense why drug users tend to report a reduced ability to feel pleasure. (Image and data taken from no. 2 on reference list.)
Bottom line, psychiatric medications don’t work as well as most people think (which is a subject to explore deeper in another article), and they work even more poorly when a patient has impaired neurotransmitter activity.
In closing, here’s something a little more hope-inspiring: the psychiatric provider I worked with would let his patients know that their brains would recover as much as they can within 18 months of abstinence.
References:
1. White, C.M., Browne, T., & Nafziger, A.N. (August 15, 2021). Inherent Dangers of Using Non–US Food and Drug Administration–Approved Substances of Abuse. American College of Clinical Pharmacology. https://accp1.onlinelibrary.wiley.com/doi/10.1002/jcph.1860
2. What is drug addiction? (July 2020). National Institute on Drug Abuse. https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/drug-misuse-addiction
More articles:
Cured of Mental Illness, Part 1
Psych Meds No Better than Street Drugs? Turns out They Have a Lot in Common